B1 Malaria
B1.1 Introduction
-
Capacities taught in this chapter
Scientific processHow are discoveries in science made?Scientific toolsWhich tools are the most appropriate for malaria research?Reading and interpretingWhat is the life cycle of the malarial parasite in its vector and its host?
How has malaria been treated in the past?
How are new methods of diagnosis discovered?Bridging science, society and the environmentHow can we prevent malaria?Quantitative skillsIs the incidence of malaria changing?
- parasite
- An organism that receives its nutrition from another organism by living in or on it and requires such a host for survival.
Malaria is a disease that has a long and complex history, the earliest recorded evidence of which dates as far back as 2700 BC.1 Wherever it spread, malaria had a severe impact on communities and nations, affecting the outcome of battles and wars and changing the course of history. Researchers have made great progress in their understanding of the disease by following scientific methods. Some risked their lives in the process. Thanks to these brave people, we now know that malaria is caused by microscopic Plasmodium parasites, which are transmitted to their hosts by the bite of female Anopheles mosquitoes. We also have developed ways to prevent and treat malaria. However, the battle is far from over. Malaria continues to be a major threat to human health around the world. Today, 200 million people in the world are infected with malaria annually and nearly half a million die from the disease.2 India is one of the countries where the malaria parasite thrives. Each year, 12 million people are infected, and 20 000 people die from malaria in India alone.3
Although records of malarial fevers date back 3000 years4, we will limit our study of malaria to more recent times: the discovery of how the disease is transmitted to a human, the history of treatment, and current diagnosis measures. We will take an interdisciplinary view of the problem that malaria presents to the human population. After a brief review of the malarial parasite, its life cycle, and geographical distribution across the globe and in India, we will learn about two scientists who worked under unusual circumstances to make fundamental discoveries about malaria. We will then explore why drug treatments against malaria are increasingly ineffective,2 and look at how malaria may be prevented by methods ranging from leveraging our knowledge of molecular biology to field surveys for public awareness. Malaria prevention is a multi-pronged approach. We will use malaria as a case study to understand a wide range of scientific tools from the microscope to field surveys. We end the chapter with a discussion on how malaria can be diagnosed and analyse a recent publication about diagnostic testing of malaria to learn how scientific articles are written.
This chapter will not be a comprehensive review of malaria and its impact on humankind, but an introduction to the problem. Each topic will help you to build specific capacities.
First test your own understanding of malaria at the start of this unit. Return to these questions after reading the whole chapter to see how your understanding has changed or deepened.
Mosquito life cycle
You may have heard that mosquitoes transmit malaria from one person to another. What do you know about the stages of a mosquito life cycle? To control the spread of malaria, it is helpful to understand this life cycle.

Figure B1.1 The mosquito life cycle. The adult lives on land but lays eggs in water. The larval and pupal stages occur in standing water.
- surface tension
- The ability of the surface layer of a liquid to resist a certain amount of external force.
Figure B1.1 shows the life cycle of the mosquito. Notice that eggs, larvae and pupae live in water, which needs to be fresh and non-flowing. Larvae and pupae have a breathing tube that breaks the surface tension of the water and allows them to breathe. The mosquito life cycle normally takes two weeks, but it can be as short as four days or as long as a month. To develop, a mosquito larva only needs a depth of about 2.5 cm in water.
The Plasmodium parasite
- Protista
- A kingdom of unicellular or simple multicellular eukaryotic organisms.
- vector (disease ecology)
- An organism that carries disease-causing microbes from one host to another. See also: host.
- host
- An organism that harbours a pathogen or a non-disease causing agent.
Malaria is one of the deadliest diseases in the world. It is caused by Plasmodium parasites, which are unicellular organisms belonging to the kingdom Protista. Plasmodium is transmitted from adult female Anopheles mosquitoes (the vector) to a human host. An infected female Anopheles mosquito transmits the parasite when it bites a human host for nutrition. Male Anopheles mosquitoes only feed on flower nectar.
As the parasite encounters different environments in its host and its vector, it passes through different stages of its life cycle. Refer to Figure B1.2 as you read about the Plasmodium life cycle and note that each stage has a name and a characteristic morphology.

Figure B1.2 The Plasmodium life cycle. Note morphological changes in the parasite as it moves between the host and the vector.
The mosquito bite

The incubation period

Entry into the blood stream

Mosquitoes take up gametocytes

Reproduction inside the mosquito

The cycle repeats
- sporozoites
- A stage in the life cycle of Plasmodium that develops in the mosquito and is transmitted to humans with the mosquito’s saliva. See also: merozoite.
- incubation period
- Time taken for symptoms to be exhibited after infection.
- asymptomatic
- Not exhibiting any symptoms.
- gametocytes (germ cells)
- Diploid reproductive cells that undergo meiosis to produce gametes. See also: gametes.
- gametes
- Haploid reproductive cells, derived from gametocytes. See also: gametocytes.
- oocyst
- A structure that develops from the zygote of a parasite like Plasmodium.
- asexual reproduction
- The mode of reproduction that does not involve the fusion of male gametes and female gametes.
- merozoites
- A stage in the life cycle of Plasmodium in which it divides in human liver cells and then infects red blood cells. See also: sporozoites.
- When an infected female Anopheles mosquito bites a person, it injects saliva containing sporozoites of Plasmodium parasites into the human’s blood stream. Sporozoites pass into the human’s liver.
- During an incubation period, sporozoites reproduce through asexual reproduction in the liver, and the infected person remains asymptomatic. The products of asexual reproduction in the liver are called merozoites. Merozoites break out of the liver cells and enter the bloodstream through the heart and lungs.
- Merozoites move into red blood cells (RBC) where they undergo many rounds of cell division (asexual reproduction). RBCs burst open every two to four days, and are permanently damaged, causing fever. Fevers begin within 10 to 15 days of initial infection.
- Some merozoites in the RBC develop into sexual forms of the parasite, called gametocytes, that circulate in the bloodstream. A mosquito ingests gametocytes in a subsequent bite.
- Gametocytes mature into male and female gametes in the mosquito’s gut. Fertilisation results in zygotes, which burrow through the mosquito’s midgut wall and form oocysts on the exterior surface.
- Thousands of active sporozoites develop inside the oocyst. The oocysts burst open, releasing sporozoites which migrate to the mosquito’s salivary glands, and the cycle continues.
- gene expression
- Process by which the information encoded in our DNA is decoded to build proteins for cellular and body functions.
The parasite undergoes many morphological changes during its life cycle stages from sporozoite, to merozoite, to gametocyte, to gamete and finally back to sporozoite. These changes are driven by changes in gene expression.
- diptera
- Insects with two wings, for example, mosquitoes and flies.
Five species of Plasmodium cause malaria in humans. P. falciparum and P. vivax are the most common in India and the most dangerous (Figure B1.3).5 The other species are P. malariae, P. knowlesi and P. ovale.6 Although we are only concerned about malaria in humans in this chapter, it is important to know there are over 500 related species that cause malaria in reptiles, turtles, birds and mammals. The parasite is carried by at least seven different families of dipteran vectors.7
Malaria in India
At the time of independence in 1947, an estimated 20–25% of the population in India was infected with malaria, with a death toll of about 0.8 million per year.8
As of 2017, India was one of five countries accounting for nearly half of all malaria cases worldwide. However, India is progressing in both prevention and treatment of malaria. According to a World Health Organization (WHO) report published in 2019, India was no longer in the top five category. In 2018, India witnessed a 28% decrease over the previous year in estimated malaria cases3 due to several factors including increased awareness, more rapid diagnosis, and treatment. The African continent suffers the largest burden for malaria.
Figure B1.3 shows the total number of cases of malaria, the number of deaths, and the number of cases caused by P. vivax and P. falciparum from 2000 to 2020.

Figure B1.3 Malaria cases in India by parasite species.
Data from WHO, World Malaria Report 2020: India continues to make impressive gains in reduction of Malaria Burden. (2020), accessed 18 January 2021, Government of India, Press Information Bureau.
- diagnose
- Identify a disease from its signs and symptoms.
- anaemia
- A condition in which red bloods cells do not function normally, usually resulting in reduced oxygen delivery to the body’s organs.
Symptoms of malaria include fever, shivers, headaches, vomiting, and general muscle pain. Fevers occur when red blood cells burst open, releasing millions of merozoites into the bloodstream. Refer to Figure B1.2 to see where that happens during the life cycle of the malaria parasite. Even though malaria is difficult to diagnose due to a lack of symptoms immediately after infection, without treatment it will progress and lead to severe anaemia, respiratory distress and multi-organ failure that can eventually result in death. Children under five are especially susceptible to malaria and the complications arising from malarial infection.
- epidemiological profile
- The disease burden in an area in terms of demographic, geographic, cultural, socioeconomic, and clinical characteristics of infected people.
Lack of awareness among citizens about malaria and increasing drug resistance create difficulties in addressing malaria. Increasing temperatures due to climate change also create new environments in which mosquitoes can thrive. Figure B1.4 shows that the distribution of the mosquito vector and the parasite species varies region by region in India, and so does the incidence of malaria. The variation in environmental conditions, parasites and vectors in turn lead to different epidemiological profiles by region.
Each community requires its own set of preventative and curative measures against malaria, suited to the environmental conditions of the area. Malaria prevention requires people from many different professions: from physicians and public health specialists, to urban planners and climate scientists.
Human action affects the natural world at many levels, and nature in turn affects our lives. Addressing the problem of malaria is therefore not straightforward. You should keep this interconnectedness in mind while reading this textbook.

Figure B1.4 Prevalence of malaria in different states of India along with vector and parasite species distributions.
Adapted from Das, A et al., ‘Malaria in India: The Center for the Study of Complex Malaria in India’, Acta Tropica 121, no. 3 (2012): 267–273, doi: 10.1016/j.actatropica.2011.11.008.
and Wangdi, K, Gatton, ML, Kelly, GC, Banwell, C, Dev, V and Clements, AC, ‘Malaria Elimination in India and Regional Implications’, The Lancet Infectious Diseases 16, no. 10 (2016): e214–224, doi: 10.1016/S1473-3099(16)30123-2.
Exercise B1.1 Interpret the Malaria data
Reading and interpretingQuantitative skillsStudy Figure B1.3 and Figure B1.4 and answer the following questions.
- Calculate the average number of deaths per year from 2000 to 2010.
- Describe the trends in the total number of cases over the period shown in Figure B1.3.
- Calculate as accurately as possible the death rate per case for 2006. What could have caused the sudden spike in cases?
- Compare the number of cases attributed to P. falciparum with those attributed to P. vivax over the period shown in Figure B1.3.
- Figure B1.4 shows the prevalence per state together with dominant parasite and dominant vector species. Use the information in Figure B1.4 to complete the following table. The first row has been completed for you.
State Prevalence Dominant parasite species Dominant Anopheles species Assam 50–150×103 P. falciparum A. minimus A. baimaii Tamil Nadu Orissa Gujarat Jammu, Kashmir & Ladakh
B1.2 Process and History of Science
Scientific process
- scientific process
- Process of gaining knowledge through observation, hypothesis formulation, hypothesis testing, analysis of obtained data, and inference from analysis.
The scientific process is often illustrated by the history of scientists and their discoveries. Here, we will explore the scientific journeys of two different scientists in very different situations, with very different resources available to them. Their goals had one common theme: to improve our understanding of malaria and in turn to help improve human health. As you read this section, try to imagine the times these scientists lived in, their motivation, and how their circumstances may have helped or hindered their mission.
Disease transmission: Ronald Ross in India
- germ theory
- The theory that diseases are caused by microorganisms called pathogens or germs.
- miasma theory
- The theory that certain diseases, especially epidemics, were caused by ‘bad air’ or miasma.
For thousands of years, people did not know what caused malaria or how it was spread. Before the development of the scientific method, the microscope or germ theory, people had a range of theories about disease spread. For example, the name malaria dates to the early 1800s, and comes from the Italian term ‘mal aria’, meaning ‘bad air’. At the time, the prevailing theory was the miasma theory. This theory proposed that diseases, such as malaria, were caused by ‘bad air’ that came from decomposing organic matter, such as the rotting of vegetation in swampy areas.
Let us step back 170 years and follow Dr Ronald Ross’s (Figure B1.5) pioneering research on how malaria was transmitted. As you read the story of Ross’s remarkable work, try to identify different steps of the scientific process that ultimately led to his discoveries.
Figure B1.5 Sir Ronald Ross.
Wellcome Images, CC-BY 4.0.
- bacteriology
- The scientific study of bacteria.
Ross was born in India in 1857, and was educated in Britain. He studied medicine, and while he was a qualified physician, he took additional courses in bacteriology and public health. Ross had a wide range of interests. He was passionate about literature, mathematics and music, and he was also a published poet.
Ross returned to India in 1881, as a member of the Indian Medical Service at a time when malaria was a major threat to human health across several continents. Ross moved from post to post in the Indian subcontinent: Madras, Burma, Baluchistan, Andaman Islands, Bangalore and Secunderabad.
- tropical medicine
- A branch of medicine that studies diseases occuring in tropical and sub-tropical regions.
During one of his holidays, Ross met Patrick Manson, who was a pioneer in the field of tropical medicine. Manson had discovered while in China, that mosquitoes act as vectors for filariasis, a disease caused by filarial worms. Manson convinced Ross that malaria was an important disease to study, and that India was a good place to do so.
- microscopy
- Using microscopes to study small objects.
- pigmented bodies
- Structures within malaria-infected red blood cells that accumulate hemozoin, a pigment produced by the malaria parasite.
At the time, research using microscopy had revealed two observations. Firstly, the malaria parasite resides inside the liver cells of infected people. Secondly, the red blood cells of infected people contain structures called pigmented bodies (Figure B1.6). The pigmented bodies arise due to hemozoin, a pigment created when the Plasmodium parasite metabolises proteins in the red blood cells. However, no one had worked out how the malaria parasites infected humans in the first place.

Figure B1.6a Pigmented bodies (indicated by arrows) seen in red blood cells of a person who has malaria.
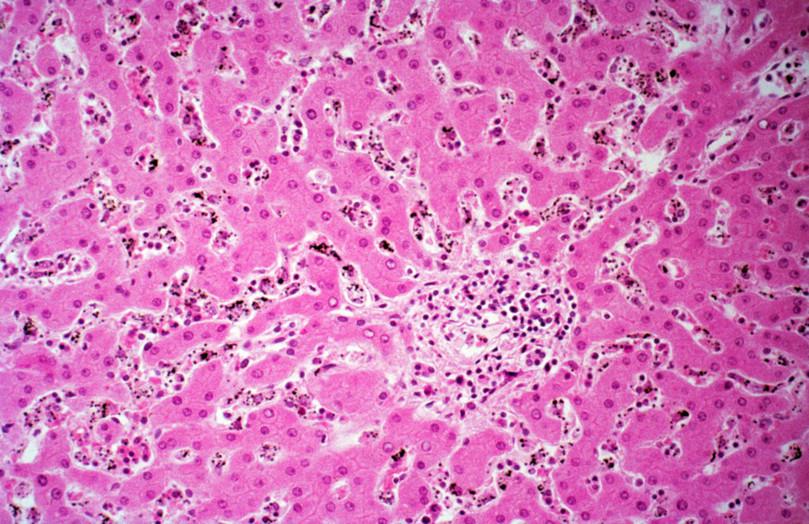
Figure B1.6b Section of liver tissue from a person with falciparum malaria. The dark spots are hemozoin.
Wellcome Collection, CC0 1.0 Universal.
- endemic
- In animals and plants, endemic means a species that belongs to and is restricted to a particular region. In a disease, endemic means occurring regularly in a certain area or among certain people, animals or plants.
Inspired by Manson’s work on mosquitoes as vectors for filariasis, Ross wondered if mosquitoes could be vectors for malaria. He began to observe mosquitoes in India and noticed that mosquitoes with dappled wings, later identified as the Anopheles species, occurred in areas where malaria was endemic. He stated his hypothesis in an 1896 letter: ‘The belief is growing on me that the disease is communicated by the bite of a mosquito … She always injects a small quantity of fluid with her bite – what if the parasites get into the system in this manner?’
- blood meal
- Food supply consisting of the blood of another organism.
In 1897, when stationed at Secunderabad Ross made a breakthrough. He managed to culture adult mosquitoes from collected larvae and then paid a malarial patient named Husein Khan to provide a blood meal for these mosquitoes. Ross then dissected the mosquitoes and viewed them using a portable microscope that he had designed himself (Figure B1.7a). He documented his observations meticulously. Pigmented bodies were visible in the digestive tract of the mosquitoes, indicating the presence of the malaria parasite. He concluded from this that the malaria parasites in the red blood cells of the person with malaria had been transmitted to the mosquitoes during the blood meal. This was the first evidence that malaria parasites could be transmitted from humans to mosquitoes. But the question remained: could the malaria parasite be transmitted from mosquitoes to humans?

Figure B1.7a The portable microscope Ronald Ross used during his research on malaria in India.
Science Museum Group Collection Online, CC-BY-NC-SA 4.0.
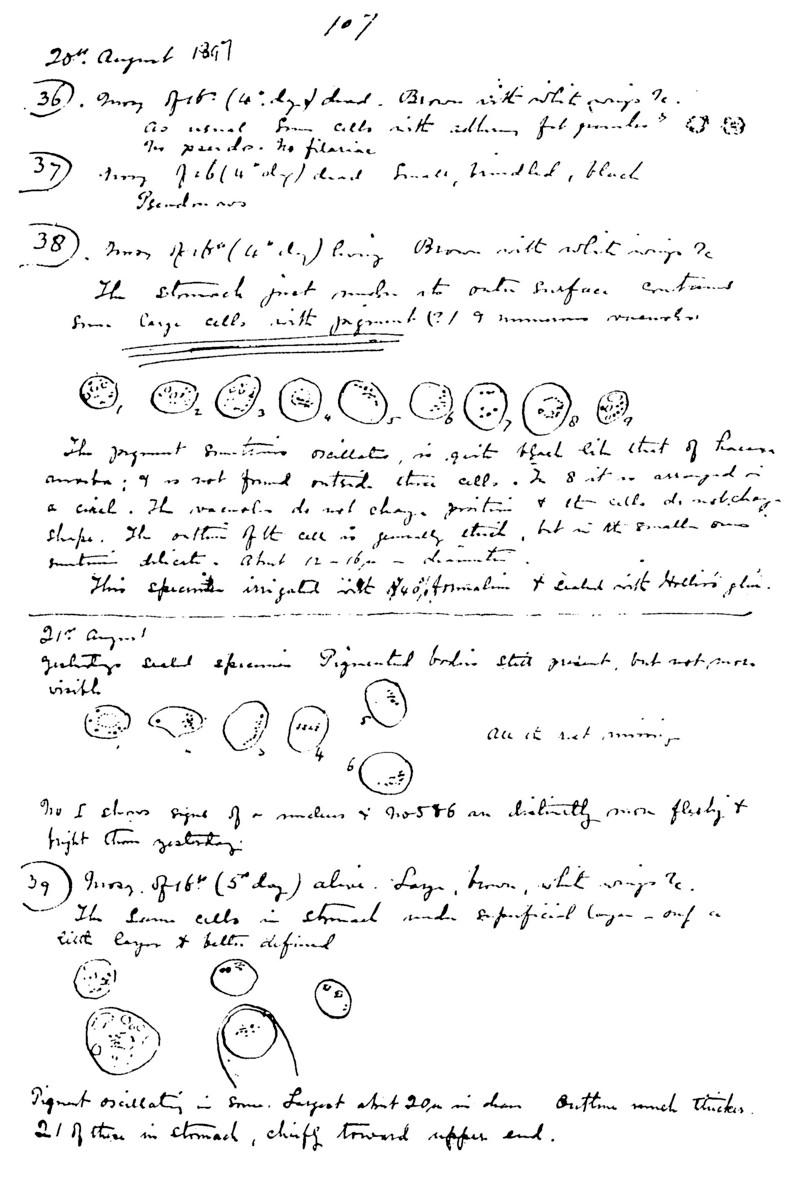
Figure B1.7b Ronald Ross’s notes.
Ronald Ross, Wikimedia Commons, public domain.
- model organism
- An organism that has characteristics that make it useful for studying various processes in a laboratory.
In 1898, Ross was posted to Calcutta, where malaria infection rates were low. He was unable to find suitable patients to continue his research, so he began to use a model organism to investigate whether the malaria parasite could be transmitted from mosquitoes to humans. He used birds to study avian malaria and found that pigmented bodies were stored in the salivary glands of mosquitoes and released into healthy birds during a blood meal,9 completing the cycle of transmission of the parasite from vector to host and vice versa. Giovanni Battista, an Italian physician, later confirmed this discovery for the human host. He showed that, in a malaria endemic area, humans protected from mosquito bites did not acquire the disease, but those who were bitten fell sick.
- epidemiology
- The study of the factors that determine presence of disease and other health conditions, and the distribution patterns of these conditions in a defined population.
- Nobel Prize
- Prize awarded to people in the fields of physiology or medicine, physics, chemistry, literature, economic sciences, and peace studies. Named after Alfred Nobel.
Ross continued his work by pioneering malaria prevention efforts around the world. He also developed mathematical models to help understand the epidemiology, which is the study of the distribution and cause of malaria. For all his work, Ronald Ross was awarded a Nobel Prize in Physiology or Medicine in 1902.10 The prize was controversial because Giovanni Battista had also done pioneering work on the human malarial parasite but did not receive the same recognition. Recognition of scientific achievement continues to be contested, not just for prizes, but also for research funding, employment, infrastructure, and so on.
- quinine
- Medicine derived from the cinchona tree that is used to treat malaria.
- active ingredient
- The component of a drug that exerts a direct effect in the diagnosis, cure, mitigation, treatment, or prevention of a disease.
Soon after the complete malaria life cycle was discovered, cinchona tree bark from Peru was identified as having curative effects on malaria patients. In the 1920s, quinine was identified as the active ingredient in the cinchona bark, and was subsequently used as an effective treatment against malaria. Less than two decades later, signs emerged that quinine’s efficacy was reducing: drug resistance was evolving!11 Variants of quinine have since been produced, and over time those too have become less and less effective against malaria. The next section describes the quest for another solution.
Exercise B1.2 Interpreting the case study on Ronald Ross
Scientific processReading and interpretingBridging science, society and the environmentScientific tools
- Explain why the microscope is an essential tool for malaria research.
- Describe two discoveries that were made possible by the development of the microscope around the time Ross began his work.
- What was the main hypothesis that Ross was trying to test in his work in India?
- List the methods he used to test his hypothesis.
- What did Ross conclude about his original hypothesis?
- Describe any difficulties Ross faced in his research and how he overcame them.
Modern chemistry and traditional medicine: Tu Youyou in China

Figure B1.8 Tu Youyou
Bengt Nyman, Wikimedia Commons, CC-BY-SA 4.0.
- western medicine
- A method of treating diseases using evidence-based practices.
Moving forward to the 1960s, a young scientist named Tu Youyou from Ningbo, China, had begun her career in pharmacy at a newly established institute, the Institute of Chinese Materia Medica. She had studied pharmacy, driven by her own encounter with tuberculosis and a desire to find new treatment options for patients. Tu received both Western medical training as well as in-depth knowledge of traditional Chinese medicines. She therefore embodied a unique combination of modern technology and ancient knowledge.12
In the late 1960s, the United States and Vietnam began a 20 year war that took place largely in the jungle regions of Vietnam. The death toll of the war was greater than 3 million.13 Nearly half of all troops engaged in the war suffered from malaria. By this time, drug resistance to quinine and its derivatives was so rampant that a new treatment was urgently needed. The Vietnamese government sought help from China to treat malaria.14
Extra reading Details make all the difference

The process of finding a drug that targets a particular disease.
Finding a drug that targets a particular disease is a long iterative process. In an iterative process, you do something again and again, with the aim of testing, refining and improving it. Many compounds are screened before reaching clinical trials on humans.
In Stage 1 a drug is discovered. Only about 250 of every 10 000 compounds will pass Stage 1.
Stage 2 is pre-clinical drug development, in which compounds are tested on animal models. Only about five of the 250 compounds tested will pass Stage 2.
Stage 3 is clinical development of the compounds that pass stage 2 screening. The five compounds undergo testing for effects on the body and safety in humans, effectiveness at treating diseases, larger scale safety and effectiveness, and long-term safety.
Regulatory approval: Finally, one compound receives regulatory approval and can be used for treating patients.
Clinical trials
Clinical development is the phase during which a drug is tested on humans. These trials are typically broken up into four phases.
- Phase I studies test the drug for safety on a small number of people.
- Phase II studies evaluate drugs found to be safe in phase I on a larger group of people to monitor side effects.
- Phase III studies account for variations within the population by testing the drug in different locations and larger populations.
- Phase IV studies take place over a longer timeframe to evaluate any long-term side effects, even after a regulatory body has approved the drug.
Tu was appointed the head of a project to search for and extract antimalarial drugs among traditional Chinese medicines. Her approach to the problem was to scour ancient Chinese texts, searching for mentions of fevers that matched malarial symptoms. Tu focused on 640 recipes for anti-malarials derived from animal and plant matter.
After two years of trial and error, Qinghao (the Chinese name for the Artemisia genus) were found to be effective at times in rodent models. However, the herb’s effects were not consistent every time. Tu Youyou returned to the ancient texts and focused on one specific sentence: ‘A handful of Qinghao immersed in two litres of water, wring out the juice and drink it all’ (Figure B1.9b). There was no mention of boiling the water (which is typical of most herbal remedies). This attention to detail was very useful. Tu hypothesised, and later showed, that heating damages the active ingredient in the plant.

Figure B1.9a In the Artemisia species, only A. annua (also known as sweet wormwood) produces the active ingredient, artemisinin.
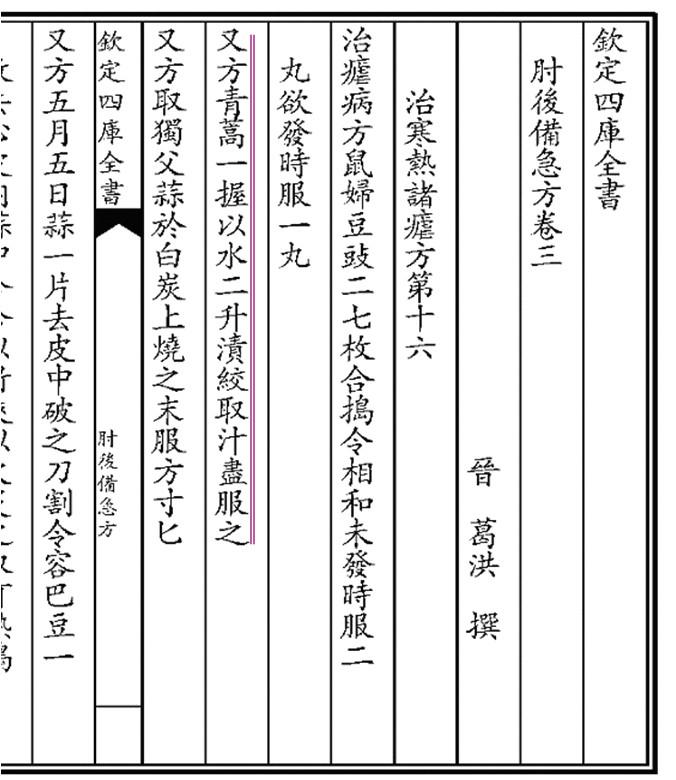
Figure B1.9b The highlighted Chinese script reads ‘A handful of Qinghao immersed in two litres of water, wring out the juice and drink it all’.
Ge Hong, Wikimedia Commons, public domain.
- clinical trial
- A stage of medical research which involves testing of a treatment on a large number of humans in a controlled manner.
Because of the urgent demand for a new medicine, Tu’s team needed to develop one within months, a much shorter timeframe than is usually required. They needed to test the safety of the active ingredient, artemisinin, in humans before they could continue to develop the medicine. To save time, Tu volunteered herself to take the medicine, along with two other members of her team. Once safety was established, clinical trials were initiated and expedited. Note that usually the development of a new drug is an iterative process that takes many years. Using traditional knowledge gave her a very helpful starting point.
Since its discovery, artemisinin and its derivatives have helped more than 200 million malaria patients recover. Tu Youyou’s story is an example of a unique interdisciplinary approach, utilising ancient Chinese texts, pharmacology, traditional chemistry, and medicine. In 2015, Tu Youyou was the first Chinese woman to win the Nobel Prize in Physiology or Medicine for her work.
Exercise B1.3 Analysing the case study on Tu Youyou
Scientific processReading and interpretingBridging science, society and the environment
- What were the training and resources that helped Tu Youyou formulate her hypotheses?
- What was her hypothesis?
- How did she test her hypothesis?
- What was her conclusion?
- What difficulties did she face and how did she overcome them?
- Identify similarities and differences between the Tu and Ross case studies in terms of their aims, approach, methods and circumstances.
Summary
We have touched on two stories that are part of a much larger whole comprising human interaction with malaria. What is striking about both stories is the connections scientists made between what they observed and what they read and heard in order to come to a plausible conclusion. Note that this process is iterative: Tu Youyou for example read many texts, experimented, then returned to the text again before she realised she should not be heating the active ingredient for it to be effective. She did all this in the face of many challenges. Ronald Ross’s story provides inspiration both because his interests were wide ranging, and because of his persistence and belief in his hypothesis that mosquitoes were the vector of the malaria parasite. We also examined the state of malaria in India, the life cycle of a parasite, and an overview of the drug discovery process.
B1.3 Preventing Malaria
Reading and interpreting Bridging science, society and the environment
Addressing the impact of Malaria on human populations requires many approaches. By controlling the mosquito vectors of malaria, we make it harder for the malaria parasite to spread to new human hosts. Without new hosts, the parasite will not be able to survive. Methods available for controlling the vector mosquito include avoidance, insecticides and genetic engineering.
Avoidance
Chemical repellents, mosquito nets, wearing clothing that covers exposed skin, avoiding stagnant water, and spraying a thin layer of oil on stagnant water are all effective strategies to avoid malaria.
Exercise B1.4 Prevention Methods
Reading and interpretingBridging science, society and the environmentRefer to Figure B1.1.
Match each of the malaria-control measures 1 to 6 in the table to its effect on the mosquito life cycle (A to E).
Malaria-prevention measure Effect on mosquito life cycle 1. Spraying oil on stagnant water A. Prevents adult mosquitoes from biting people while sleeping 2. Sleeping under mosquito nets B. Kills adult mosquitoes 3. Taking quinine tablets C. Disrupts host-seeking behaviour of adult mosquitoes 4. Covering bare skin in the evening D. Prevents the larvae from breathing and breaks the life cycle 5. Rubbing a scented oil on your skin E. Prevents adult mosquitoes from biting exposed skin 6. Spraying insecticide inside the house
Public awareness of disease transmission is vital to the success of prevention programmes.3 What do you think a public awareness campaign includes? How would you go about implementing one? Refer to section B1.4 on how field surveys help gather information, and may in turn inform public awareness campaigns.
Insecticides
Insecticides are chemicals that kill pest insects. One of the most widely used insecticides is dichloro-diphenyl-trichloroethane (DDT) which was used during World War II to effectively control malaria and typhus fever among civilians and military troops.
Extra reading The tumultuous history of DDT
Paul Muller, a Swiss scientist, was awarded the Nobel Prize in 1948 for discovering the use of DDT as a contact poison that killed several insects. In his Nobel lecture, Paul Muller listed several desirable qualities of a contact poison:
- great insect toxicity
- rapid onset of toxic action
- little or no mammalian or plant toxicity
- no irritant effect and no or only a faint odour (in any case not an unpleasant one)
- the range of action should be as wide as possible and cover as many Arthropoda as possible
- long, persistent action, in other words, good chemical stability
- low price (= economic application).
Several insecticides were tested, but DDT satisfied all these criteria except that it had a slow onset of action. Note that various factors go into designing a novel insecticide.
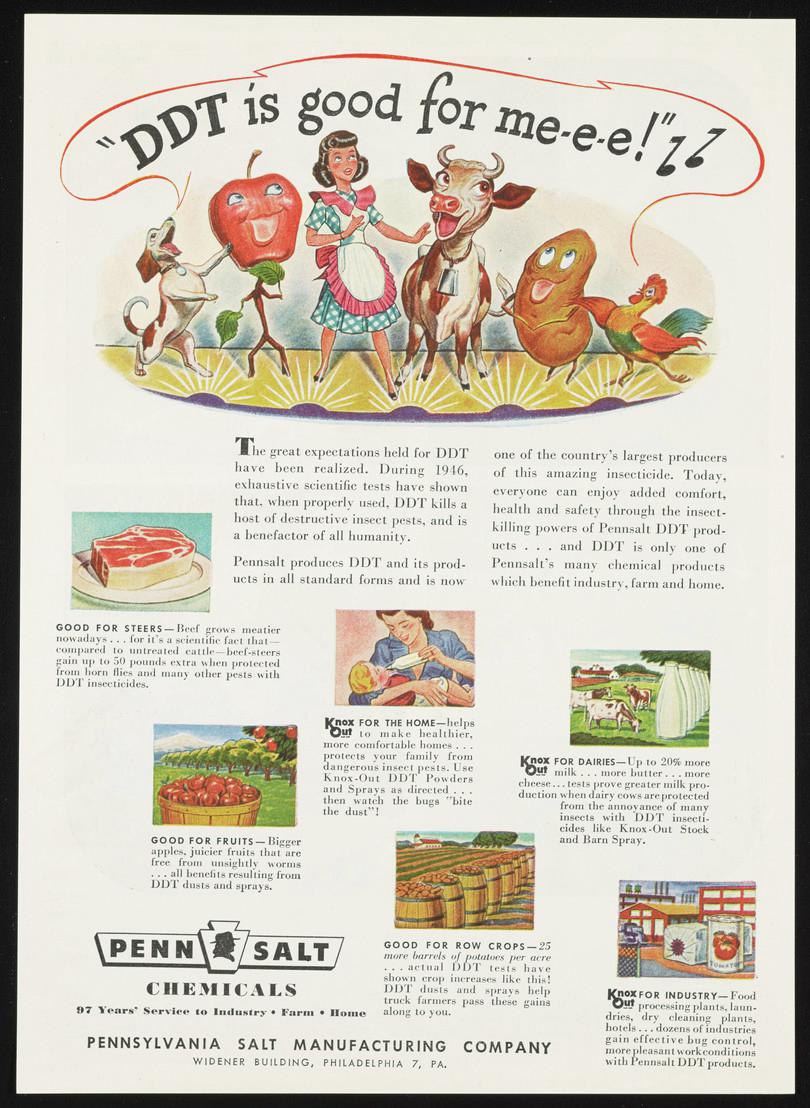
Figure B1.10 Time magazine ad from 1947 depicting DDT as a miracle product for widespread use as an insecticide.
Courtesy of Science History Institute, public domain.
Following its success as a pesticide, DDT was widely used in homes as well as agricultural fields, especially in the USA. DDT was also sprayed over entire cities in the USA to kill flies, as they were thought to transmit polio. A Time magazine advertisement shows the popularity of DDT in the 1940s (Figure B1.10). Indeed, DDT was used to kill other non-mosquito pests of important crops.
- zooplankton
- Tiny invertebrate animals that drift in the water.
- trophic level
- The position an organism occupies in a food chain.
- biomagnification
- The process of accumulation of toxins in organisms as we move higher up a food chain.
In 1962, Rachel Carson, an American marine biologist, wrote a book called Silent Spring in which she showed how DDT accumulates in the tissues of living organisms and is magnified as it moves along the food chain. DDT sprayed on agricultural farms can get into lakes and rivers due to surface water runoff. Zooplankton take up the DDT, passing it to fish. The fish are in turn eaten by birds of prey. DDT causes thinning of the eggshells produced by these birds. The chicks do not develop properly in the eggs and do not hatch, leading to a severe decline in bird populations. The concentration of DDT in each trophic level increases, with highest concentrations in the top predators. This is known as biomagnification.
- carcinogen
- Any substance that causes cancer.
- endocrine disruptor
- Natural or artificial chemicals that disrupt hormonal (endocrine) function.
DDT is considered a human carcinogen, and is an endocrine disruptor. This means that exposure to DDT can disrupt normal hormonal functions in our body, and it is associated with increased risk of breast cancer.15 The discoveries of the negative effects of DDT on the environment and human health lead to its banning in 1972. Rachel Carson questioned the dominant wisdom that DDT is harmless and revolutionised the environmental movement. Nevertheless, DDT is still used in several parts of Africa and India to control malaria. In 2006 the WHO permitted limited usage of DDT for indoor spraying.
As you can see, the use of DDT for the control of malaria has been a complex story. Initially hailed as a breakthrough for disease prevention, it was later banned due to its harmful effects. Now it is making a return in certain situations. This illustrates the way that scientific knowledge develops. The discovery process is continuous, building on what we know as new data comes available. In science, we are always ready to embrace new findings as they come and also to acknowledge that our initial findings might be incomplete or incorrect. Science is a continual search for improved knowledge and understanding. By its very nature it proceeds by steps based on improved techniques and tools.
India is the largest producer of DDT in the world, manufacturing around 3000 metric tonnes annually.16 Due to mass spraying, many Anopheles species have developed resistance to DDT in several regions. For example, A. culicifacies is resistant to DDT in several parts of India, and A. fluviatilis has grown resistant to DDT in Central India, and Maharashtra, while it is still susceptible in Odisha.2 How some mosquito species become resistant to DDT, and certain other species show varied amounts of resistance in different regions, are important questions.

Figure B1.11 DDT concentration increases at each trophic level due to the process of biomagnification (ppm = parts per million; ppb = parts per billion).
Adapted from Al-Jawhari, IFH, ‘Degradation of Pollutants Using Advanced Ecomaterials’, in Handbook of Ecomaterials, eds L Martínez, O Kharissova O and B Kharisov, pp. 495–515 (Cham: Springer, 2017). doi: 10.1007/978-3-319-48281-1_29-1.
Exercise B1.5 DDT and Biomagnification
Bridging science, society and the environmentQuantitative skillsA farmer sprays DDT onto crop plants, and it runs off into the nearby lake. A fish in the pond swallows some water containing zooplankton, and now has 0.1 µg/g of DDT in its body.
If a kite (a bird) eats around 500 g of this fish in one day, how much DDT does the kite consume per day?
Vaccines against malaria
Vaccines have been very effective in controlling diseases. Examples of diseases that have been successfully controlled by vaccines are polio, smallpox and diphtheria. This section gives a brief overview of what a vaccine is, and how a vaccine against malaria may be developed.

Figure B1.12 Adaptive immunity acquired through vaccination.
How does your body’s immune system work?
- macrophage
- A type of cell produced by the immune system that engulfs and breaks down pathogens.
- antibody
- A Y-shaped protein produced by the body’s immune system that recognises and binds to specific antigens and deactivates them.
- antigen
- A protein, usually on the surface of a pathogen, that elicits the body’s immune response.
The immune system is a collection of cells and organs that defend the body from attack by invaders or pathogens. An infectious agent, also known as a pathogen, has proteins that are detected as being ‘foreign’ by the host. The foreign proteins are called antigens. When the body detects antigens, a type of immune cell called a macrophage engulfs the foreign infectious agent and generates antibodies that are specific to each antigen. Antibodies are Y-shaped proteins (illustrated in Figure B1.12), produced by a type of cell called B cells, that will specifically bind an antigen. Each antibody will only bind to a specific antigen. Once the antibody binds to the antigen, the immune system recognises the interaction and it can mount a response to the invader.
How does a vaccine work?
A vaccine is a preparation made of biological matter that confers immunity against a particular disease. Note that vaccines are preventative in nature, and drugs are treatments. The vaccine generally consists of an antigen made from a weakened or inactivated version of the pathogen. Once this weakened version is in the host, the immune system will produce antibodies to the antigens.
- acquired or adaptive immunity
- The second, stronger immune defence that prevents pathogens from attacking the body and retains a memory of previous infection for a quicker response to subsequent infections.
Vaccination, as illustrated in Figure B1.12, essentially generates a long-term memory of the pathogen, so the body knows how to deal with the pathogen on the first real encounter. This is called acquired or adaptive immunity. Acquired immunity prevents illness if the pathogen enters the body again. It can last months to years, depending on the vaccine.
The specificity between antigen and antibody is exploited in many biochemical applications, including disease diagnostics, as we will see later in the research highlight. There are other kinds of vaccines that work by delivering the antigen via more indirect methods, but the general principle of acquired immunity always holds. To learn more about the history of vaccines and how they work, visit The History of Vaccines.
Though malaria has been studied for hundreds of years, there is no commercially available vaccine against it. Unlike many other diseases such as chicken pox, exposure to Plasmodium does not confer complete acquired immunity. The reasons why the immune response is limited in the case of malaria are not known. The life cycle of the parasite is complex, and it can produce continuously varying antigens quickly. If adaptive immunity is acquired to one antigen, it may not work for another antigen from the same pathogen. This makes it difficult to develop a vaccine against malaria.
Vaccines must undergo rigorous testing in clinical trials to ensure that they are safe in the short and long term. Only one malaria vaccine has completed Phase III clinical trials, and received approval by the WHO in late 2021 for widespread use. The vaccine, known as Mosquirix, provides modest protection against malaria in young infants. A total of four doses of the vaccine are administered before the age of three. The vaccine significantly increases the benefits of using a combination of prevention methods, including mosquito bed nets.17 Three African nations, Malawi, Ghana and Kenya, conducted pilot studies to test the efficacy of the vaccine.18
Summary
In this section, we looked at different approaches to tackle and prevent malaria. We can prevent mosquitoes from biting humans by using repellents, nets, and environmental awareness. We can also try to eradicate the vector by using insecticide. Though it was not discussed in this chapter, genetically modifying the mosquito so that it doesn’t spread the disease is also being explored. We could develop a vaccine to provide an effective antibody response to malarial antigens, and we can use antimalarial drugs that help in combating the parasite. Countries often adopt a multi-pronged approach to eradicating malaria. While immense scientific advances are made in all of these areas, it is important to note that the malarial parasite and the vector can evolve resistance to drugs or insecticides. Such resistance can cause enormous damage to the environment. Solutions for preventing malaria also has to be country/region specific, keeping socio-economic challenges in mind as well, as one solution does not fit all problems.
B1.4 Scientific tools
Scientific tools
- public health
- The study of the health of a population (community, town, city, state or country) as a whole.
In section B1.3 we discussed different measures we can take to prevent malaria. In this section we will explore other scientific tools that can be used to understand and tackle malaria. We use malaria as a case study to build our understanding of these basic scientific tools: microscopy, experimental design, and field surveys. At the cellular level, microscopy can be used to detect the parasite in patient blood samples. Experiments test and develop drugs and vaccines to treat malaria and to protect people from malaria. Field surveys provide information for public health surveillance and malaria awareness programmes.
Microscopy: a tool for disease diagnosis
There are two paths for diagnosing malaria:
- laboratory tests detect malarial antigens
- direct observation of a blood sample enables a health care worker to see the parasite.
The World Health Organization (WHO) has developed a microscopy training course and may serve as a further resource to learn about the practical aspects of malaria diagnosis.
- staining
- A technique used to highlight certain components of a cell or microorganism under the microscope with the help of a stain or dye.
To examine a blood sample, the health care worker needs a microscope, because the parasites are very small. Areas without access to advanced laboratories commonly use microscopic diagnosis. The blood sample is first turned into film on a microscope slide and stained for the parasite, as shown in Figure B1.13. Staining selectively colours the parasite, so that it looks darker compared to its surroundings and can be detected more easily. Once the microscopist has identified the stained parasite in the sample, the malaria diagnosis is confirmed.

Figure B1.13a Steps to making a blood film. By advancing the cover slip, the blood is gently smeared into a layer, so that light can pass through the sample and individual cells can be identified. Depending on the requirement, either a thin or thick blood smear is needed. A thick smear detects whether you have malaria or not. A thin smear tells which species of Plasmodium you have.
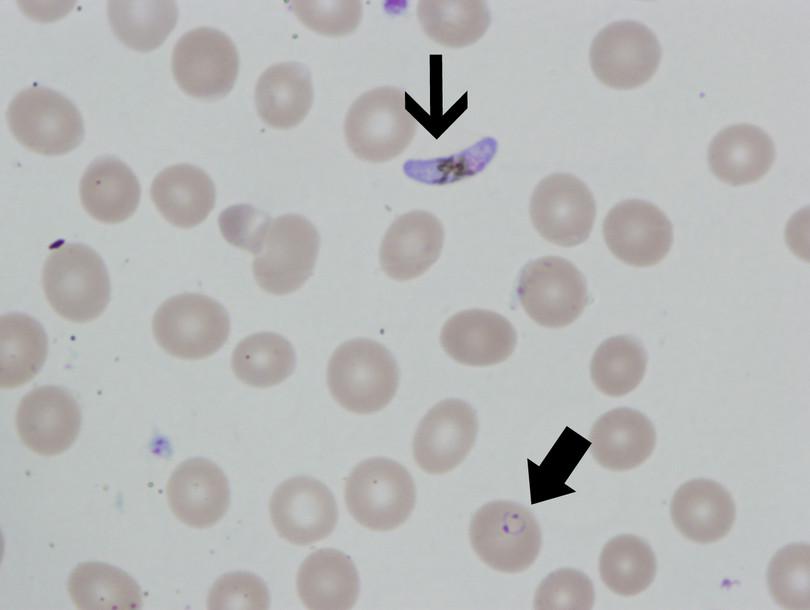
Figure B1.13b Stained blood sample, with arrows pointing to ring forms and an oblong gametocyte typical of P. falciparum.
Jenkayaks, Wikimedia Commons, CC-BY-SA 3.0.
The most commonly used microscope is the optical light microscope. While optical light microscopes come with a wide range of functionality, the basic features remain the same.
The microscope provides a frame for magnifying lenses and a stage on which to place the sample (see Figure B1.14). The function of the primary components of a microscope are:
- Lenses: A microscope has two lenses: the eyepiece that you look through, and the objective, that focuses light and magnifies the sample. Generally, objectives range from 10× to 100×. 10× means that the lens magnifies the object 10 times larger than its original size.
- Light: In the simplest microscope, a mirror reflects ambient light onto the sample. More advanced microscopes use a light bulb to illuminate the sample and a condenser to concentrate the light on the sample.
- Stage: The microscope slide is placed on the stage. The light source and lenses sit directly above or below the sample.

Figure B1.14 A compound microscope and its constituents. A compound microscope allows a higher level of magnification with the help of multiple lenses in the objective lens and eyepiece.
Three parameters are important while making observations under a microscope: magnification, resolution and contrast.
- Magnification is the ratio of an object’s image apparent through the eyepiece to its actual size. To obtain the total magnification of the object you are viewing, we multiply the power of the objective (10×, 40× or 100×) by the power of the eye piece, typically 10×. So, if you are using a 40× objective, and 10× eyepiece, the image you see through the microscope is 400 times larger than its actual size.
- Resolution is the minimum distance two points can be distinguished as two separate points. Higher resolution will allow you to see finer details of a sample, and is determined primarily by the objective lens.
- Contrast is the difference in brightness between dark and light areas of an image. One can increase contrast by making dark areas darker and light areas lighter. Many microscopes are equipped with a condenser (shown in Figure B1.14), which allows light to be focused onto the specimen, and increase the contrast as a result.
Many different kinds of microscopes have been developed, from the simple self-assembled paper, the Foldscope, to extremely sophisticated ones, but all of them rely on the same basic principle of magnification described here. In fact, the Foldscope was originally designed to help diagnose parasitic diseases such as malaria, dengue, and African sleeping sickness, in the developing world. The Foldscope is very light for transport, doesn’t damage easily, and is much cheaper than larger microscopes. It has become a portable tool for any aspiring scientist who wants to explore the microscopic world.

Figure B1.15 The Foldscope, a lightweight paper microscope that you can assemble yourself and carry in your pocket and that costs less than 400 rupees. It can magnify objects up to 2000 times for viewing.
Sockenpaket, Wikimedia Commons, CC-BY-SA 4.0.
The microscope is a fundamental tool for many studies in biology. As illustrated in Figure B1.16, life exists across different length scales. Why should length scales matter? Suppose you are interested in understanding the Plasmodium life cycle. You may want to compare the sizes of sporozoites, merozoites, gametocytes, gametes and zygotes. Length scales will be important for your investigation.
The type of microscope you use depends on the length scale you want to study, as illustrated in Figure B1.16.
The importance of lengths scales are highlighted in Primer I on numbers and scales.

Figure B1.16 Lengths scales in biology.
Field surveys: a tool for disease surveillance
- disease surveillance
- Collecting and analysing large amounts of data about various aspects of disease prevalence, generally used during epidemics and pandemics.
Disease surveillance is an important tool in controlling malaria and other diseases. Health officials collect and analyse data to monitor disease prevalence, evaluate the effectiveness of preventive measures, and allocate resources for healthcare.
Suppose you are a public health official who has been assigned the task of malaria prevention in your village. Before reading further, pause and consider what steps you might take. Consider also that different methods may be undertaken to obtain information about the community. How would you decide which would be the best method to use?
Survey design is very important. Suppose the government decides to provide every household with mosquito nets. It is important to first understand the nature of the problem, to understand, for example, whether people know how malaria is transmitted. Will they understand why they should use a mosquito net?
A guideline of the steps you may consider taking before you begin a survey are listed below. The steps are outlined with a specific idea in mind: to understand people’s practices and knowledge of mosquitoes and malaria. The ultimate purpose is to use the information that is gathered to design a malaria prevention programme. While these guidelines refer to a survey that requires interaction with a human population, field surveys are not limited to humans. One can conduct surveys to observe plant and animal abundance and/or behaviour too.
Designing and implementing a malaria prevention initiative using a field survey
- Define the scope:
- Why am I doing this survey? You should have one primary purpose for the survey. Other information may emerge, but it is important to focus on the primary purpose.
- Who is it for?
- Become more knowledgeable:
- Research existing information about this community, or other communities that may be relevant to your study.
- Determine the sample, and the sample size:
- If it is not feasible to survey every individual or household, what is the sample and sample size that would be representative of the community? Would two households represent the community, or should you sample ten households from varying income brackets?
- Determine the method of survey:
- Questionnaires can be in a written format (completed by the individual) or in an oral format (administered as an interview by the survey team). Questionnaire design is a key aspect of collecting information. You may consider what language to use, the length and complexity of the questions, whether you will collect subjective or objective data. While subjective data may include individuals’ experiences and opinions, objective data is based on facts or observations. Finally, you must consider how you will analyse this data, and ultimately use it to implement malaria prevention.
- Physical observation and investigations may help you to observe the problem you are investigating.
- Other considerations:
- Once you have collected data, it is important to analyse and interpret it. For example, if 95% of people claim they have never had malaria in an area that is dominated by Plasmodium carrying mosquitoes, what are possible interpretations of this data? Statistical analysis will help you summarise large amounts of information. Consult a statistician who understands the context.
- When you interpret your survey results, you need to understand the interacting parameters. For example, how does economic background relate to education, infrastructure, and interaction with the mosquito vector?
- Talking to people in the community will help you implement a programme. A survey design and its implementation must be informed by knowledge of the local norms and customs of the population.
- Suggest and implement solutions:
- Public awareness campaigns may help you to implement solutions you have designed, taking into account the community’s customs and knowledge.
- Implementation often requires concerted effort by public health officials and the public at large.
- Follow up on a regular basis to verify the success of the programme.
- Consult all stakeholders:
- Talk to community members such as doctors, nurses, public health officials and the population at large to get a clearer picture of the problem. Good communication may help to implement and sustain future prevention programmes.
Exercise B1.6 Design your own survey
Scientific toolsBridging science, society and the environmentDivide your class or study circle into groups and conduct a small survey in your neighbourhood, apartment building, village or school.
Here is a list of suggestions:
- Do people who use water filters in their homes actually benefit from them?
- Which household water sources are the most economical (borewells, open wells, rainwater harvesting, government pipeline, tankers)?
- What proportion of people use sustainable transport to travel to their workplace?
While designing the survey, make a distinction between subjective and objective questions.
Subjective question: What do different communities do to keep mosquitoes away?
The answer may vary depending on who you ask.
Objective question: What is the incidence of malaria or mosquito population in a region?
There is a clear answer no matter who you ask.
List three other subjective and objective questions that you can ask.
After conducting the survey, return and present the results to the other groups. In what contexts can the results of each group be put to use?
Behavioural tools to understand biology: How do mosquitoes detect humans?
Malaria is transmitted by the bite of female Anopheles mosquitoes. But how does the mosquito actually find a human to bite? Scientists are still seeking answers to this question. The simple task of finding a host or food is actually a complex behaviour.
Scientists study behavioural questions from a proximate and an ultimate perspective. Nikolaas Tinbergen, a Dutch biologist in the 1970s came up with a framework to examine behaviour from different perspectives (Table B1.1). Proximate level questions on this topic could relate to how a behaviour developed, and the developmental changes in a behaviour. Ultimate level questions could relate to the evolutionary history of that behaviour, and the current utility of that behaviour.
| How questions | Why questions |
|---|---|
| Mechanism (causation) | Ontogeny (development) |
| Adaptive value (function) | Phylogeny (evolution) |
Table B1.1 Tinbergen’s four categories of questions to explain animal behaviour.
Take mosquitoes finding a human host as an example for studying foraging behaviour. What are the questions that can be asked, based on Table B1.1?
- reproductive success
- The number of offspring surviving and reaching reproductive maturity, measuring how successfully a gene passes on from one generation to the next.
- Mechanism: How do mosquitoes detect human hosts?
- Ontogeny: Do mosquitoes get better at finding humans over their lifetime?
- Phylogeny: How did the host-searching behaviour evolve? Is it similar in other mosquito species?
- Adaptive value: How does host-seeking behaviour increase a mosquito’s reproductive success? Are there any costs associated with this behaviour?
- proboscis
- (invertebrates) Organ used for feeding. 2. (vertebrates) Elongated nose.
Mosquitoes use various sensory organs at different distances from the human host. They can detect carbon dioxide generated by our breath from 30 to 40 feet away! They follow the CO2 gradient towards a host, using their compound eyes to track the host. Once they come closer, they use our body heat and odour (particularly lactic acid) to land on us. Next, they use receptors present on the antenna, proboscis (insect tongue) and other mouth parts to detect and identify the right host.19 Heat or lactic acid alone don’t seem to elicit a host-searching behaviour, but CO2 seems to augment the attractiveness of these cues.20 Various custom built equipment can be used to find out how mosquitoes detect human hosts.
Research highlight Rapid diagnostic testing of malaria
In many areas of India, access to health care, infrastructure and training for health care workers is limited. Using a microscope to diagnose malaria requires a microscope and someone who is trained in preparing the sample and identifying the parasite in a blood smear.
- rapid diagnostic test
- Quick and simple tests usually used to detect parasite-based infections.
- point-of-care testing
- Testing that occurs on-site, where the patient is.
- mouth swab
- Collection of saliva and epithelial cells from inside the cheek to test for the presence of pathogens or other substances.
Another diagnostic tool is a rapid diagnostic test (RDT), which can be used at point-of-care, meaning that it does not require a blood sample to be sent to a lab for further analysis. This is helpful to people living in remote areas. The RDT is a quick, efficient and accurate method for screening for malaria. If the disease can be diagnosed quickly, treatment starts early and the patient recovers faster. Non-invasive ways of obtaining the patient’s sample, such as a mouth swab or urine sample, are advantageous as they do not require highly trained personnel.
- immunoassay
- A test that measures presence and concentration of antigens through the use of antibodies.
How do RDTs work? The most common RDTs are in the form of an immunoassay, which involves detecting the interaction of an antibody with an antigen. The antibody is specific to the pathogen. The antigen–antibody interaction is linked to some type of visible detector. For a better understanding of what an antibody is, refer to section B1.3.

![The image shows how components of a blood sample travel across a sheet with three bands containing antibodies and colloidal gold, a detector molecule. Antigens (Ag) in the blood will attach to the mobile antibodies (Ab) in the first band and move forward. The second band, called the test band, has stationary antibodies, to which some of the Ag-Ab complexes bind. The remaining complexes travel further and attach to the stationary antibodies in the control band.]()
Figure B1.17 A rapid diagnostic test, testing for the presence of disease with the help of capillary flow and antigen–antibody binding.
- immunochromatographic antigen detection (lateral flow test)
- A test that uses the principle of capillary flow, by which antigen–antibody complexes can migrate across a surface, to test for presence of antigens.
Figure B1.17 shows an example of an RDT that is an immunochromatographic antigen detection test. What does this long name mean? Study the detailed steps of the test below.
- lysed
- Broken (or burst) cell.
- chromatography
- A technique used to separate components of a mixture by allowing them to flow across a surface.
- Cells from a patient’s fluid sample are lysed open and allowed to run onto the RDT strip. You can see the sample moving in Figure B1.17. This process is known as chromatography.
- If the sample contains the parasite antigen, as it travels, an antibody linked to a detector molecule (usually something coloured) will be picked up along with the sample. Now the antigen (Ag) is complexed with the labelled antibody (Ab).
- The sample continues to move past the first band, which is the test band. If the sample contains the antigen, the Ag-labelled Ab will be captured on the test band by the pathogen-specific antibodies that are fixed on the band.
- To ensure that the test sample migrated properly, a second band, the control band, is found further from the test band. As the sample crosses the control band, the antibody will be captured, also colouring the control band.
- By the end of a prescribed time period, two coloured bands indicate a positive diagnosis. If only the control band is coloured, it indicates a negative diagnosis. If only the test band is coloured, but not the control band, the test is invalid.
Pregnancy tests and even point of care tests for Covid-19 rely on the same principle as described above.
- cerebrospinal fluid
- A colourless body fluid found in and around the brain and spinal cord that cushions the brain from sudden mechanical shocks.
In India, the most common RDT for malaria uses HRP2 as a target antigen. HRP2 is a protein that is found in the cytoplasm of the parasite. The protein is also released into the host’s body fluids such as blood, cerebrospinal fluid and urine. HRP2 is not an essential protein for parasite survival. While the HRP2 target antigen has been used successfully for malaria diagnosis, it is limited in its scope in India for two reasons: a) HRP2 is present only in P. falciparum, so other species cannot be detected; and b) since HRP2 is not essential, several studies have identified P. falciparum strains in which the HRP2 gene has been lost (or deleted) over some generations.21 These reasons highlight the need to search for another antigen that can be used to detect all species of Plasmodium found in India.
The guided paper by Amreen Ahmed et al.22 (ICMR-National Institute of Research in Tribal Health in Jabalpur) identifies one antigen (glutamate dehydrogenase) that has the potential to be used for RDTs for malaria in India. The article is annotated to facilitate the reading of this work. As you read through the work, make note of how this journal article is organised. How do the authors introduce the problem they are trying to address?
Summary
In this section we used the example of malaria to demonstrate some scientific tools: a microscope, field surveys, and behavioural experiments. We briefly reviewed the role of each part of the microscope and subsequently discussed how it can be used to diagnose malaria. Some scientific questions cannot be answered using experiments. Field surveys can be used to study different communities to find out what people know about malaria and what interventions they may accept. Field surveys allow us to gain knowledge of a system by observation and question-answering. The third tool considered briefly how we can investigate host-seeking behaviour in mosquitoes. Finally, the research highlight explained how rapid diagnostic testing (RDT) can be used to diagnose diseases such as malaria and coronavirus.
Now that you have finished this chapter, take a moment to check how your understanding of malaria has improved. Revisit the questions you answered at the start of the chapter. Use the critical thinking questions as prompts to check whether your understanding improved.
B1.5 Quiz
Question B1.1 Choose the correct answer(s)
Malaria is one of the deadliest diseases in the world. According to the World Health Organization report, the incidence of new malaria cases in India in 2018 was 6.7 million.
If the total population of India was 1.3 billion in 2018, what percentage got malaria?
- To calculate percent incidence, divide the incidence by total population and multiply by 100.
- Make sure you have counted zeros in the billions and millions properly!
- Check where the decimal point is placed.
- There is more than one way to write the answer.
Question B1.2 Choose the correct answer(s)
Using the 2018 population figure, if 7% of the population were malaria free, how many million were free of malaria?
- Multiply total population of India in 2018 by 7 and divide by 100 OR multiply total population of India by 0.07.
- Always double check your answers when you are dealing with decimals and large numbers.
- Always double check your answers when you are dealing with decimals and large numbers.
- There is more than one way to write the answer.
Question B1.3 Choose the correct answer(s)
Consider a person who is 70 kg and has a total blood volume of 5 litres. There are typically 5 million RBCs per 1 µl of blood.
How many RBCs are there in the person’s body?
- 5 litres of blood is equivalent to 106microlitres (µl). The rest is simple multiplication.
- There is more than one way to represent the correct answer.
- Make sure you are careful with where you place the zeros, and decimal points.
- Make sure you are careful with where you place the zeros, and decimal points.
Question B1.4 Choose the correct answer(s)
DDT was banned in 1972 because of its adverse effects on the environment and on humans and animals. Overuse of DDT also causes resistance in mosquitoes. Table B1.2 gives the amount of DDT used in public health as well as in the agricultural sector in India in the 1960s and 1970s.
| 1960 | 1965 | 1966 | 1967 | 1968 | 1969 | 1970 | 1971 | 1972 | 1973 | 1974 | 1975 | 1976 | 1977 | 1978 | |
| Malaria incidence (×106) | 0.10 | 0.15 | 0.28 | 0.27 | 0.35 | 0.69 | 1.31 | 1.43 | 1.93 | 3.17 | 5.16 | 6.46 | 4.74 | 4.14 | |
| DDT used in public health (tonnes) | 21 007 | 6671 | 2762 | 3045 | 5821 | 6401 | 6205 | 7350 | 7034 | 6821 | 6700 | 7250 | 7250 | 9051 | 6800 |
| DDT used in agriculture (tonnes) | 600 | 2400 | 2400 | 2400 | 2400 | 2400 | 2400 | 2400 | 2400 | 2880 | 2934 | 2450 | 3000 | 2450 | 4720 |
Table B1.2 Amount of DDT used in public health and in the agriculture sector.
Data from Sharma, VP and Mehrotra, KN, ‘Return of Malaria’, Nature 298, no. 5870 (1982): 210–210, doi: 10.1038/298210a0.
How did the incidence of malaria and DDT usage in public health change between 1965 and 1980?
- Track the trend in DDT usage in public health over the period. Track the trend in incidence of malaria over the same period. Relate the two trends.
- There is some variation in DDT usage over the years, but that’s not significant. You can see malaria increasing.
- Although the data for 1977 and 1978 shows decreasing malaria incidence, it is not enough to make a claim that malaria incidence had actually decreased.
- The data clearly shows higher amounts of DDT doesn’t help to eradicate malaria. This hints at the possibility of developing resistance towards DDT.
Question B1.5 Choose the correct answer(s)
If DDT reduces mosquito populations, what can explain the overall increase in malaria incidence despite a steady rise in DDT usage between 1966 and 1972?
- Mosquitoes and other insects are likely to evolve resistance to prolonged usage of insecticides like DDT.
- Even if we use a large quantity of DDT, it may kill some mosquitoes, but is not going to solve the issue of resistance.
- DDT toxicity is not area specific. Insecticides should work across the globe.
- Mosquitoes are known to develop a gene mutation that confers resistance towards DDT.
Question B1.6 Choose the correct answer(s)
Many parasites besides malaria cause vector-borne diseases and share similar life cycles. The diseases they cause range from sleeping sickness to leishmaniasis.
All of the diseases listed above occur primarily in tropical regions. What are the possible reasons for this?
- Most vectors, like mosquitoes and ticks, prefer warm weather and the climate in tropical regions provides suitable conditions for breeding.
- Wherever vectors are found, the pathogen is also likely to be found.
- Mosquito larvae hatch in shallow still water.
- Parasites have a specific host range, for example avian Plasmodium will not infect the human host unless some evolutionary event(s) take place.
B1.6 References
-
Cox, FEG, ‘History of the Discovery of the Malaria Parasites and their Vectors’, Parasites & Vectors 3, no. 5 (2010). https://doi.org/10.1186/1756-3305-3-5 ↩
-
Wangdi, K, Gatton, ML, Kelly, GC, Banwell, C, Dev, V and Clements, ACA, ‘Malaria Elimination in India and Regional Implications’, The Lancet Infectious Diseases 16, no. 10 (2016): e214–224, doi: 10.1016/S1473-3099(16)30123-2. ↩ ↩2 ↩3
-
World Health Organization, World Malaria Report 2019 (Geneva: WHO 2019). Licence: CC BY-NC-SA 3.0 IGO. ↩ ↩2 ↩3
-
Dagen, M, ‘History of Malaria and Its Treatment’, in Antimalarial Agents pp. 1–48 (Amsterdam: Elsevier, 2020) doi: 10.1016/B978-0-08-101210-9.00001-9. ↩
-
Ghosh, SK and Rahi, M, ‘Malaria Elimination in India: The Way Forward’, Journal of Vector Borne Diseases 56, no. 1 (2019): 32–40, doi: 10.4103/0972-9062.257771. ↩
-
Rutledge, GG et al., ‘Plasmodium Malariae and P . Ovale Genomes Provide Insights into Malaria Parasite Evolution’, Nature 542, no. 7639 (2017): 101–104, doi: 10.1038/nature21038. ↩
-
Martinsen, ES, Perkins, SL and Schall, JJ, ‘A Three-Genome Phylogeny of Malaria Parasites (Plasmodium and Closely Related Genera): Evolution of Life-History Traits and Host Switches’, Molecular Phylogenetics and Evolution 47, no. 1 (2008): 261–273, doi: 10.1016/j.ympev.2007.11.012. ↩
-
Shiv, L, Sonal GS and Phukan PK, ‘Status of Malaria in India’, Journal of Indian Academy of Clinical Medicine 5, no. 1 (2000): 19–23. ↩
-
Malaria Site, ‘Ronald Ross’, 25 February 2015, accessed 7 April 2020. ↩
-
The Nobel Prize, ‘The Nobel Prize in Physiology or Medicine 1902: Robert Ross Biographical’, accessed 7 April 2020. ↩
-
Faurant, C, ‘From Bark to Weed: The History of Artemisinin’, Parasite : Journal de La Société Française de Parasitologie 18, no. 3 (2011): 215–218, doi: 10.1051/parasite/2011183215. ↩
-
The Nobel Prize, ‘The Nobel Prize in Physiology or Medicine 2015: Tu Youyou Biographical’, accessed 7 April 2020. ↩
-
Spector, RH, ‘Vietnam War 1954–1975’, Britannica, accessed 7 April 2020. ↩
-
Su, X and Miller, LH, ‘The Discovery of Artemisinin and the Nobel Prize in Physiology or Medicine’, Science China Life Sciences 58, no. 11 (2015): 1175–1179, doi: 10.1007/s11427-015-4948-7. ↩
-
Soto, A and Sonnenschein, C, ‘Endocrine Disruptors: DDT, Endocrine Disruption and Breast Cancer’, Nature Reviews: Endocrinology 11 (2015): 507–508, doi: 10.1038/nrendo.2015.125. ↩
-
Van den Berg, H, Manuweera, G and Konradsen, F, ‘Global Trends in the Production and Use of DDT for Control of Malaria and Other Vector-Borne Diseases’, Malaria Journal 16, no. 401 (2017), doi: 10.1186/s12936-017-2050-2, accessed 7 April 2020. ↩
-
World Health Organization, ‘WHO recommends groundbreaking malaria vaccine for children at risk’, accessed 08 October 2021. ↩
-
World Health Organization, ‘Q&A Detail: Malaria: The Malaria Vaccine Implementation Programme (MVIP)’, accessed 7 April 2020. ↩
-
Raji, JI and DeGennaro, M, ‘Genetic Analysis of Mosquito Detection of Humans’, Current Opinion in Insect Science 20 (2017): 34–38, doi: 10.1016/j.cois.2017.03.003. ↩
-
Potter, CJ, ‘Stop the Biting: Targeting a Mosquito’s Sense of Smell’, Cell 156, no. 5 (2014): 878–881, doi: 10.1016/j.cell.2014.02.003. ↩
-
Poti, KE, Sullivan, DJ, Dondorp, AM and Woodrow, CJ, ‘HRP2: Transforming Malaria Diagnosis, but with Caveats’, Trends in Parasitology 36, no. 2 (2020): 112–126, doi: 10.1016/j.pt.2019.12.004. ↩
-
Ahmad, A, Verma, AK, Krishna, S, Sharma, A, Singh, N and Bharti, NS, ‘Plasmodium Falciparum Glutamate Dehydrogenase Is Genetically Conserved across Eight Malaria Endemic States of India: Exploring New Avenues of Malaria Elimination’, PLOS ONE 14, no. 6 (2019): e0218210, doi: 10.1371/journal.pone.0218210. ↩

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}